
AI might move at the speed of trust, but new research in JAMA Network Open shows that trust only moves at the speed of accuracy.
The study had a solid setup. To determine the factors currently driving patient trust in AI, researchers presented 3,000 U.S. adults with a pair of hypothetical AI-assisted visits for a moderate-risk rash.
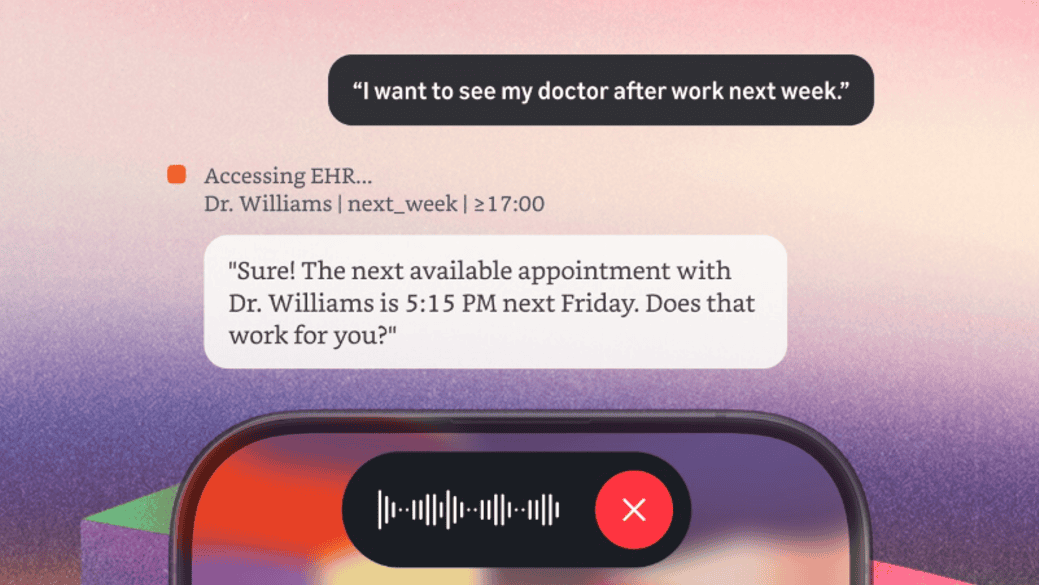
- Each visit had six randomized attributes, such as whether or not a doctor was present, how well the AI performs relative to human clinicians, and various AI governance mechanisms.
- Participants chose their preferred visit, rated their trust in the diagnosis, and explained their choice with a single-sentence explanation for their choice. Here’s a good example of the potential visits.
AI performance came out on top by a wide margin. Respondents cared more about how well the AI performs than FDA approval, governance, and even having a doctor in the room.
- The biggest difference came from AI performing better than a specialist, which increased the likelihood of choosing that visit by 32.5%.
- AI performing at the same level as a specialist boosted visit preference by 24.8%, slightly more than having AI that performs as well as a general practitioner (19.1%).
- Having an actual doctor present surprisingly only swayed visit preference by 18.4%.
Governance factors also moved the needle. They just didn’t move it much.
- FDA approval for the AI increased visit preference by a modest 11.1%.
- Mayo Clinic AI certifications apparently carry just as much weight – also coming in at 11.1%.
- Local hospital certifications for the AI only gave visits a 7.8% lift.
AI data quality was important. It just wasn’t as convincing as AI performance.
- AI that had nationally representative training data boosted visit preference by 11.9%, but it was interesting to see that disclosing bias in the training data had no effect versus not providing any data details.
The written explanations told the same story. Respondents cited AI performance and clinician involvement as the primary reasons for their choices, with many of them expressing comfort with AI as a tool – but not as a standalone decision-maker.
The Takeaway
Widespread AI adoption requires patient trust, and this study did a great job highlighting the specific areas that should be prioritized for building it.




{kind=link}