

Rock Health just dropped its H1 digital health funding overview, and the halftime report shows a market that knows where it’s going, even if the way it gets there keeps changing.
Here’s H1 2026 by the numbers:
- Digital health startups raised $7.4B across 244 rounds (up $1B from H1 2025).
- Median round size climbed from $12M to $14M, the highest since 2022.
- 19 companies raised 20 mega-rounds, accounting for 45% of all capital invested.
That last stat is starting to look familiar. Capital concentration was the headline of the Q1 report, and the trend hasn’t let up.
- Just over 8% of rounds absorbed nearly half the capital, and some companies aren’t even waiting a full year between nine-figure checks.
- Garner Health’s $100M Series E landed three months after its Series D, and Aidoc grabbed its second $150M in under a year.
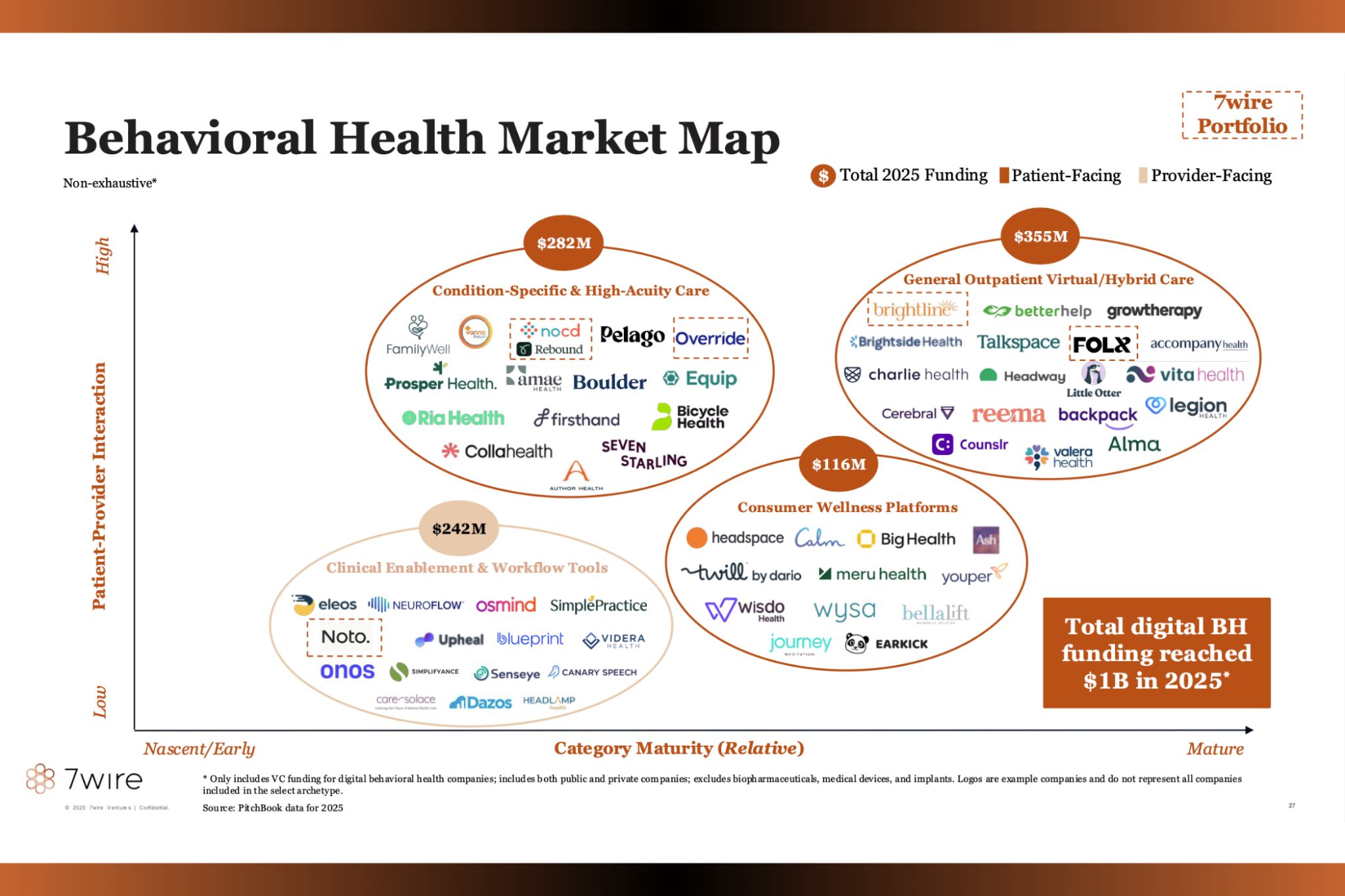
Mental health is still the belle of the ball. It was the top-funded clinical indication for the seventh straight year, led by Talkiatry ($210M) and Grow Therapy ($150M).
- Weight management took the silver on the back of the insatiable appetite for GLP-1s.
- Both categories share a secret weapon: 64% of their H1 raisers go direct-to-consumer, versus 29% of digital health overall.
The IPO drought is creeping back. After seven exits last year, 2026 hasn’t produced a single digital health IPO, and Oura’s S-1 is the only one on file.
- This year’s exit action is all M&A. H1 saw 115 acquisitions, including 71 in Q2 alone (the busiest quarter since 2021), with revenue cycle management consolidating fastest.
Where are all the moats? The H1 report’s big question was what actually counts as a durable advantage now that “we have AI” no longer moves the needle.
Rock Health landed on four answers and one graphic:
- founders with real domain expertise (sharpens product and buyer relationships)
- platforms scaling to own more workflows (and more context to coordinate tasks)
- hands-on delivery (forward-deployed engineers are officially a healthcare job)
- network effects (every new partnership builds on the last so competitors can’t catch up)
The Takeaway
AI made digital health products easier to build than ever, which means the products themselves are no longer the moat. Investors are looking for the same fundamental roots – teams, trust, and traction – but the routes to find them are shifting faster than ever.







{kind=link}