

Digital diabetes management tools found themselves in the hot seat after a blistering study from the Peterson Health Technology Institute suggested that several leading solutions don’t provide significant clinical benefit, especially relative to their cost.
That conclusion naturally had many digital health advocates sharpening their pitchforks, but first let’s start by unpacking PHTI’s research and findings.
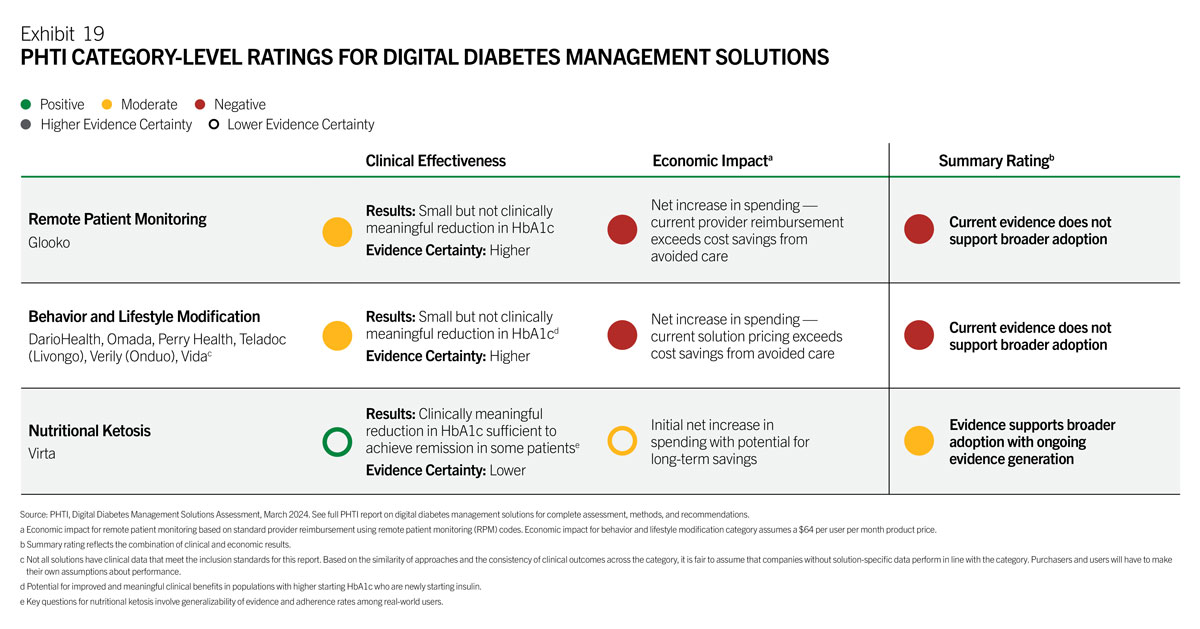
The analysis had two main endpoints: clinical effectiveness and economic impact. PHTI reviewed 1,100+ articles, including 120 submitted by the companies being evaluated, then offered ratings across three categories – remote patient monitoring, behavior / lifestyle modification, and nutritional ketosis. This chart summarizes the results beautifully.
- On the clinical side, PHTI found that these tools deliver small reductions in HbA1c (0.23 to 0.60 percentage points) compared to usual care, as well as limited long term durability of the improvements.
- On the economic side, PHTI concluded that each of the three product categories led to a net increase in spending, with total reimbursement and program investment exceeding any cost reduction from avoided care (the ketosis category carried an asterisk for its potential to cut costs over the long term).
Those findings led to plenty of blowback, including an excellent rebuttal from the Digital Therapeutics Alliance and a flurry of press releases from the companies in the report.
The DTx Alliance’s rebuttal centered around three primary issues:
- The limited selection of solutions overlooks a large portion of the diabetes tools on the market, and that it’s misleading to give generalized conclusions based on a small sample when many products can demonstrably improve clinical and economic outcomes.
- The report’s reliance on predictive models rather than actual cost studies overlooks real-world evidence, particularly concerning products like Dario, which has independent studies demonstrating reductions in both costs and hospitalizations.
- It might have made sense for PHTI to list any of the nation’s 9,000 endocrinologists (diabetes experts) as authors or advisors. It’s tough to beat their pointed suggestion: “Had there been expertise in this evaluation, they may have considered the broader scope of diabetes management like reductions in hypo- and hyperglycemic events, in addition to the reduction of A1C levels.”
The Takeaway
Embracing debate is essential if the industry wants to improve, and even if there was room for improvement in PHTI’s methodology, it definitely succeeded in its goal of refocusing attention on the clinical and economic impact of digital innovations.

{kind=link}